Due to the high body weight of our patients and their nature as flight animals, the treatment of fractures in equine medicine represents a particular challenge. However, continuous advances in veterinary medicine mean that, unlike several decades ago, a bone fracture is no longer necessarily a death sentence for the affected horse.
Through many years of experience and ongoing professional development, the Bargteheide Equine Clinic has specialized in the surgical treatment of fractures.
Key parameters that are decisive for the prognosis of a horse with a fracture include the bone involved, the size and weight of the horse, the fracture configuration, and whether the fracture is open or closed. Overall, the prognosis is significantly better in lighter horses with fractures of the distal limb than in heavier horses with fractures of the proximal limb. Comminuted fractures are more difficult to manage than simple longitudinal fractures. Open fractures, in which the skin is disrupted, generally carry a poorer prognosis because bacteria entering through the wound frequently lead to infection, particularly when plates and screws are used for osteosynthesis.
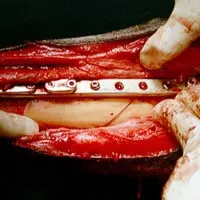
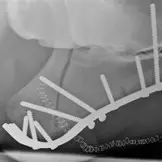
Splint bone fractures are the most common fractures in horses. In these cases, the prognosis following surgery is usually favorable, as the cannon bone bears the main load of the limb. Typically, the blind-ended distal fragment of the splint bone is amputated. In closed fractures of the proximal third of the splint bone, plate osteosynthesis may be a reasonable treatment option. Open splint bone fractures in the distal region can usually be treated successfully by surgery, whereas open fractures involving the splint bone head are generally not treated surgically but are allowed to heal conservatively. In rare cases, total resection of a splint bone may be unavoidable.
Fractures of the distal phalanx present a surgical challenge due to its location within the hoof capsule. Fractures of the solar margin or wing of the distal phalanx are treated with strict stall rest, corrective shoeing, and hoof casting. Longitudinal fractures of the distal phalanx have a less favorable prognosis because of joint involvement and the associated risk of osteoarthritis; these fractures may be treated either by screw fixation or by casting.
Fractures of the middle phalanx are rare and are usually comminuted fractures with poor healing prospects. In some cases, the horse can be salvaged by arthrodesis of the proximal interphalangeal joint.
Fractures of the proximal phalanx often occur as stress fractures in the mid-shaft region and can be treated with screw fixation and additional casting, with generally favorable healing prospects.
Fissures of the proximal phalanx (proximal phalangeal fissures) can be managed with stall rest and, if necessary, cast fixation. Ideally, however, osteosynthesis is also performed in these cases to provide greater stability of the fissure and to counteract the development of subchondral bone cysts. Overall, these fissures usually have a good prognosis.
Fractures of the proximal long bones, such as the radius and humerus, as well as the tibia and femur, represent a major surgical challenge. In these cases, prognosis is highly dependent on the horse’s body weight, the type of fracture (closed or open; transverse, spiral, or comminuted), and any involvement of adjacent joints.
An exception is fractures of the ulna or elbow region. These fractures occur frequently in young horses and, depending on the fracture pattern, carry a guarded to favorable prognosis.
The decision to surgically treat a fracture should be made carefully through discussion between the surgeon and the owner, taking animal welfare, economic considerations, and surgical feasibility into account.
Surgical fracture, treatment is particularly challenging due to the following factors:
The high body weight of the horse results in substantial mechanical stress on the fracture site, both during recovery from anesthesia and throughout the healing phase. Unlike in human medicine, weight bearing on the injured limb cannot be reduced by prolonged recumbency or the use of walking aids. Additional stabilization by casting is not feasible, particularly in the proximal limb, meaning that immediate load-bearing stability must be achieved following surgery. To reduce mechanical stress after fracture surgery, a suspension system (sling support) is available at our clinic. This system supports part of the horse’s body weight using a flexible harness, allowing the horse to move freely within the stall and to lie down safely.
A distinction is made between simple transverse fractures, spiral fractures, and comminuted fractures. In the latter, healing prospects are generally poor due to insufficient load-bearing stability. In open fractures, as opposed to closed fractures, the skin is breached either by sharp bone fragments or by the external traumatic force. These fractures also generally carry a poor prognosis due to bacterial contamination of the wound.